Decoding Neck Pain: By the Medical Team, Sapiens Pain Hospital

By the Medical Team, Sapiens Pain Hospital
Neck pain is a common health issue, typically associated with the degeneration of cervical spinal structures, muscles, and joints, or resulting from prolonged poor posture.
1) Primary Causes of Neck Pain
- Myofascial Strain: Muscle and ligament tension or inflammation due to poor posture.
- Cervical Facet Arthropathy: Degeneration of the small joints in the neck.
- Cervical Disc Herniation & Radiculopathy: Herniated discs leading to nerve root compression (pinched nerves).
- Cervical Spinal Stenosis: Narrowing of the spinal canal.
- Whiplash-Associated Disorder (WAD): Injuries resulting from sudden acceleration-deceleration (e.g., car accidents).
- Red Flags (Dangerous Causes): Infections, malignancy (cancer), fractures, or vascular diseases.
2) Evaluation and Diagnostic Imaging
The process begins with a detailed medical history and physical examination to screen for "red flags." According to the American College of Radiology (ACR) guidelines, X-rays or MRIs are not always necessary during the initial phase unless there are clear neurological deficits, severe trauma, or suspicion of high-risk conditions.
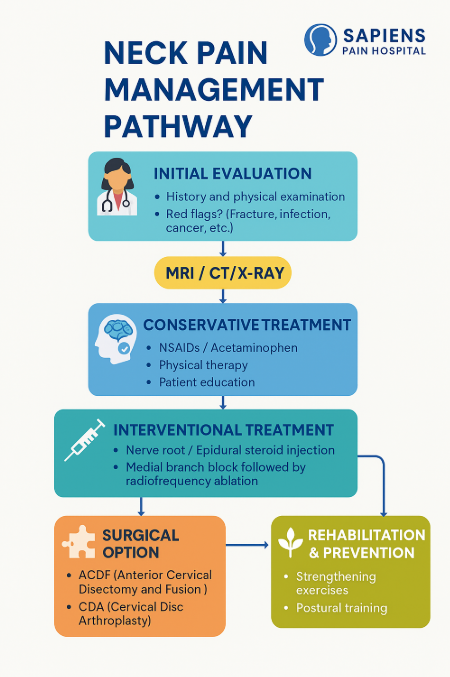
3) Recommended First-Line Treatments
- Education and Behavioral Modification: Adjusting workstation ergonomics (monitor height and seating), avoiding prolonged neck flexion (looking down), and performing regular stretching.
- General Analgesics: Use of Acetaminophen or NSAIDs as clinically appropriate.
- Physical Therapy (JOSPT/APTA Guidelines): Evidence-based programs focusing on neck and scapular strengthening, manual therapy (joint mobilization), and movement control exercises.
4) Modern Specialized Treatments (Popular in the U.S.)
4.1 Selective Nerve Root Block / Cervical Epidural Steroid Injection
This is suitable for patients with radiculopathy (pain radiating down the arm caused by nerve compression). It reduces inflammation and provides short-to-medium-term pain relief, allowing patients to participate more effectively in physical therapy. The procedure is performed under C-arm (fluoroscopy) guidance for maximum precision.
4.2 Medial Branch Block & Radiofrequency Neurotomy (RFA)
This approach targets pain originating from the facet joints. It begins with a diagnostic block of the medial branch nerves; if the patient responds well, RFA is considered. RFA uses thermal energy to disrupt pain signals at specific points. International multidisciplinary reports support its efficacy in properly screened patients.
If non-surgical treatments fail and there is clear evidence of nerve compression, surgeons may recommend:
- ACDF: Anterior Cervical Discectomy and Fusion.
- CDA: Cervical Disc Arthroplasty (Artificial Disc Replacement). Long-term follow-up studies in the U.S. report that CDA provides excellent overall outcomes and may reduce the likelihood of secondary surgeries in certain patient groups by preserving motion.
Current medical standards advise against the long-term use of opioids for non-severe neck pain. Instead, the focus is on multimodal treatment combined with physical rehabilitation, quality sleep, and mental well-being.
6) When to Consult a Specialist Immediately
Seek professional medical attention if you experience:
- Progressive muscle weakness or radiating numbness.
- Loss of bowel or bladder control.
- Fever or rapid, unexplained weight loss.
- Severe trauma/accidents.
- Persistent pain lasting more than 6–8 weeks despite proper self-care.


