Chronic Cough in Children: Allergies or Asthma?
Last updated: 14 Jul 2026

Chronic Cough in Children: Allergies or Asthma?
When a child coughs continuously for several weeks—especially at night, after running, in cold weather, or so severely that it disrupts their sleep—parents often worry: "Is my child suffering from allergies, or is it the start of asthma?"
This is one of the most common questions in pediatric examination rooms. A chronic cough in children rarely stems from a single cause. Crucially, a "cough" does not always equate to asthma. Conversely, some children with asthma may not present with a distinct wheezing sound every time; instead, their condition might manifest as a chronic cough, night coughing, or coughing after exercise.
According to the CHEST guidelines, a child under the age of 14 is considered to have a "chronic cough" when they cough every day for more than 4 weeks—not just a lingering cough for a few days after a common cold. Therefore, if your child has been coughing continuously for over a month, particularly if it disrupts their sleep, school, or play, or if it is accompanied by other abnormal symptoms, they require a systematic medical evaluation rather than a revolving door of different cough syrups.
Why Do Children Develop a Chronic Cough?
Coughing is a natural defense mechanism that helps clear mucus, dust, pathogens, or irritants from the respiratory tract. After catching a cold, some children may continue to cough for a while because their bronchial lining remains hypersensitive to triggers.
However, if the cough persists beyond 4 weeks, pediatricians will look for other underlying causes, such as:
How Do Allergies Cause a Chronic Cough?
Allergies that trigger a chronic cough in children usually involve the upper airway, particularly allergic rhinitis.
Children in this group often experience:
The ARIA guidelines (international guidelines for allergic rhinitis) emphasize that nasal allergies and asthma are closely linked because they represent a connected airway disease. Children with allergic rhinitis should always be evaluated for asthma, especially if they also experience coughing after running, night coughs, wheezing, or chest tightness.
Asthma in Children Doesn’t Always Start with a Wheeze
Asthma is a chronic inflammatory disorder of the airways that causes bronchial hyperresponsiveness to various triggers. A child may experience coughing, wheezing, chest tightness, difficulty breathing, easy fatigue, or severe coughing fits after exercise, exposure to cold air, dust, smoke, or viral infections.
According to GINA 2025, an asthma diagnosis should be based on a history of characteristic respiratory symptom patterns that vary over time and in intensity, together with the documentation of variable expiratory airflow limitation (such as spirometry or bronchodilator responsiveness testing once the child is old enough to cooperate).
Children suspected of having asthma often exhibit specific coughing patterns, such as:
What is the Difference Between Allergies and Asthma?
When to See a Doctor
If your child coughs every day for more than 4 weeks, you should take them to see a doctor for a proper diagnosis—especially if the cough disrupts their sleep, prevents them from playing or exercising, occurs regularly after running, is accompanied by wheezing/shortness of breath/chest tightness, or if there is a family history of asthma and allergies.
Red Flag Signs (Seek immediate medical attention if the cough is accompanied by):
Diagnostic Tests for a Chronic Cough
A proper evaluation begins with a detailed medical history that goes far beyond asking "how many days has the child been coughing?"
A pediatrician will investigate:
Treatment for Allergy-Induced Chronic Cough
If the cough is linked to allergic rhinitis, treatment focuses on reducing nasal mucosal inflammation and postnasal drip. This may include:
⚠️ Key Takeaway: Allergy treatment requires time and consistency. Parents should not abruptly stop medications just because symptoms improve after a few days if the doctor has prescribed a continuous course, as controlling nasal inflammation effectively reduces the cough reflex and restores quality sleep.
Treatment for Pediatric Asthma
If the symptoms point to asthma, the physician will assess severity, symptom frequency, nighttime awakenings, rescue inhaler usage, activity limitations, and exacerbation history. Modern asthma management does not rely solely on rescue bronchodilators during an attack; instead, it prioritizes long-term controller medications to suppress airway inflammation, thereby preventing flare-ups and reducing long-term risks.
GINA emphasizes that comprehensive asthma care must include:
Household Triggers Parents Often Overlook
Children with allergy- or asthma-induced chronic coughs are far more sensitive to their environment than we realize. Common household triggers include:
Do Cough Medicines Help?
Cough syrups might make parents feel like they are actively treating the illness, but in cases of chronic cough, they do not address the root cause. If the cough stems from allergic rhinitis, the nose needs treatment. If it stems from asthma, the airways need control. If it is caused by chronic bronchitis, infection, or specific lung diseases, treatment must target those conditions.
Using multiple cough medicines consecutively without a diagnosis simply delays proper care. International guidelines firmly advocate for accurate diagnosis prior to therapy rather than relying on cough suppressants as a blanket solution.
Frequently Asked Questions (FAQs)
Q: Does a night cough always mean my child has asthma?
A: Not necessarily. Night coughing can be caused by allergic rhinitis, postnasal drip, asthma, GERD, or post-infectious bronchial hyperresponsiveness. However, if the night cough co-occurs with coughing after running, wheezing, chest tightness, or a family history of allergies, an asthma evaluation is highly recommended.
Q: Will a child with allergic rhinitis eventually develop asthma?
A: Not every child will, but nasal allergies and asthma are deeply connected. A child with allergic rhinitis—especially one who coughs after physical exertion, coughs at night, or experiences wheezing—should be evaluated for both conditions. It should not be dismissed as "just a simple nasal allergy."
Q: Does every child with a chronic cough need a chest X-ray?
A: Not always. For a cough lasting over 4 weeks, a pediatrician will decide based on history and physical findings. If red flag signs are present—such as chronic productive cough, prolonged fever, weight loss, shortness of breath, or abnormal lung sounds—a chest X-ray plays a vital role. Chronic cough guidelines advise targeted diagnostic testing rather than ordering tests indiscriminately.
Q: My child coughs every time they run. Should they stop exercising?
A: Absolutely not. Coughing after running can be a sign of exercise-induced bronchoconstriction or poorly controlled asthma. The child needs a proper medical evaluation and treatment. The ultimate goal of asthma care is to allow the child to exercise, play sports, and live a normal life—not to restrict their activities.
A chronic pediatric cough deserves careful attention, as it can range from poorly managed allergic rhinitis to asthma or other respiratory conditions. As a quick rule of thumb: if the cough is accompanied by nasal congestion, clear discharge, sneezing, itchy nose, and frequent throat-clearing, think allergic rhinitis. If it happens at night, after running, causes easy fatigue, chest tightness, or wheezing, think asthma. Keep in mind that a child can have both. Effective management does not mean "stopping the cough temporarily"—it means finding the root cause, controlling inflammation, eliminating triggers, mastering proper medication techniques, and ensuring continuous follow-up.
If your child has been coughing for more than 4 weeks, if the cough disrupts their sleep or exercise, or if it occurs alongside wheezing and other warning signs, please consult a pediatrician. Early, targeted care ensures your child sleeps better, plays harder, learns more effectively, and faces fewer flare-ups in the future.
⚠️ Emergency Warning: If your child exhibits severe breathing difficulties, blue-tinted lips (cyanosis), severe lethargy, blood in their cough, unexplained weight loss, chronic fever, or rapidly deteriorating symptoms, please go to the nearest emergency room immediately.
Sapiens Hospital
Move Better:Live Better
Tel. 02-111-3703
References
Chang AB, Oppenheimer JJ, Irwin RS, et al. Managing Chronic Cough as a Symptom in Children and Management Algorithms: CHEST Guideline and Expert Panel Report. CHEST. 2020.
Morice AH, Millqvist E, Bieksiene K, et al. ERS guidelines on the diagnosis and treatment of chronic cough in adults and children. European Respiratory Journal. 2020.
Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention, 2025 Update.
National Heart, Lung, and Blood Institute. 2020 Focused Updates to the Asthma Management Guidelines.
Bousquet J, et al. EAACI-endorsed ARIA 2024–2025 guidelines for allergic rhinitis.
Kanjanawasee D, et al. Chronic cough management: Practical guidelines and PICO-based evidence for treatment. 2024.
When a child coughs continuously for several weeks—especially at night, after running, in cold weather, or so severely that it disrupts their sleep—parents often worry: "Is my child suffering from allergies, or is it the start of asthma?"
This is one of the most common questions in pediatric examination rooms. A chronic cough in children rarely stems from a single cause. Crucially, a "cough" does not always equate to asthma. Conversely, some children with asthma may not present with a distinct wheezing sound every time; instead, their condition might manifest as a chronic cough, night coughing, or coughing after exercise.
According to the CHEST guidelines, a child under the age of 14 is considered to have a "chronic cough" when they cough every day for more than 4 weeks—not just a lingering cough for a few days after a common cold. Therefore, if your child has been coughing continuously for over a month, particularly if it disrupts their sleep, school, or play, or if it is accompanied by other abnormal symptoms, they require a systematic medical evaluation rather than a revolving door of different cough syrups.
Why Do Children Develop a Chronic Cough?
Coughing is a natural defense mechanism that helps clear mucus, dust, pathogens, or irritants from the respiratory tract. After catching a cold, some children may continue to cough for a while because their bronchial lining remains hypersensitive to triggers.
However, if the cough persists beyond 4 weeks, pediatricians will look for other underlying causes, such as:
- Allergic rhinitis (Nasal allergies)
- Asthma
- Post-infectious bronchial hyperresponsiveness
- Sinusitis
- Gastroesophageal reflux disease (GERD)
- Foreign body aspiration
- Pertussis (Whooping cough)
- Tuberculosis or other specific lung diseases
How Do Allergies Cause a Chronic Cough?
Allergies that trigger a chronic cough in children usually involve the upper airway, particularly allergic rhinitis.
Children in this group often experience:
- Clear runny nose and nasal congestion
- Sneezing, itchy nose, itchy eyes, and frequent nose rubbing
- Intermittent snoring
- Postnasal drip: Mucus dripping down the back of the throat, causing frequent throat-clearing, dry coughs, or worsened coughing at night and in the morning.
The ARIA guidelines (international guidelines for allergic rhinitis) emphasize that nasal allergies and asthma are closely linked because they represent a connected airway disease. Children with allergic rhinitis should always be evaluated for asthma, especially if they also experience coughing after running, night coughs, wheezing, or chest tightness.
Asthma in Children Doesn’t Always Start with a Wheeze
Asthma is a chronic inflammatory disorder of the airways that causes bronchial hyperresponsiveness to various triggers. A child may experience coughing, wheezing, chest tightness, difficulty breathing, easy fatigue, or severe coughing fits after exercise, exposure to cold air, dust, smoke, or viral infections.
According to GINA 2025, an asthma diagnosis should be based on a history of characteristic respiratory symptom patterns that vary over time and in intensity, together with the documentation of variable expiratory airflow limitation (such as spirometry or bronchodilator responsiveness testing once the child is old enough to cooperate).
Children suspected of having asthma often exhibit specific coughing patterns, such as:
- Coughing at night that wakes them up
- Coughing after running or strenuous play
- Coughing in cold weather or when exposed to dust/smoke
- Coughing repeatedly after every cold
- A family history of allergies, asthma, eczema, or allergic rhinitis
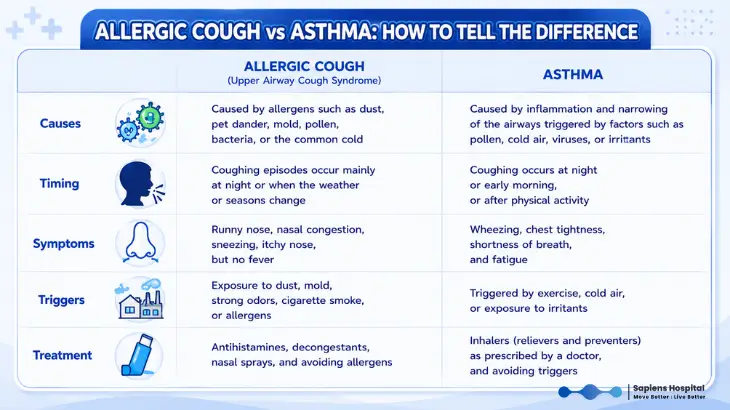
What is the Difference Between Allergies and Asthma?
- If it is Allergic Rhinitis: Symptoms are predominantly centered around the nose and throat. The child will experience nasal congestion, clear discharge, sneezing, itchy nose/eyes, postnasal drip, frequent throat-clearing, and coughing when lying down or waking up. They usually breathe comfortably, have no distinct wheezing, and can run and play almost normally.
- If it is Asthma: Symptoms are primarily related to the bronchi. The child will have coughing fits, night coughs, coughing after exercise, easy fatigue, chest tightness, or wheezing. Symptoms flare up during colds or upon exposure to cold air, dust, smoke, or allergens. Some children may simply seem to "cough easier than others," but a detailed examination will reveal airway hyperresponsiveness or lower airway inflammation.
When to See a Doctor
If your child coughs every day for more than 4 weeks, you should take them to see a doctor for a proper diagnosis—especially if the cough disrupts their sleep, prevents them from playing or exercising, occurs regularly after running, is accompanied by wheezing/shortness of breath/chest tightness, or if there is a family history of asthma and allergies.
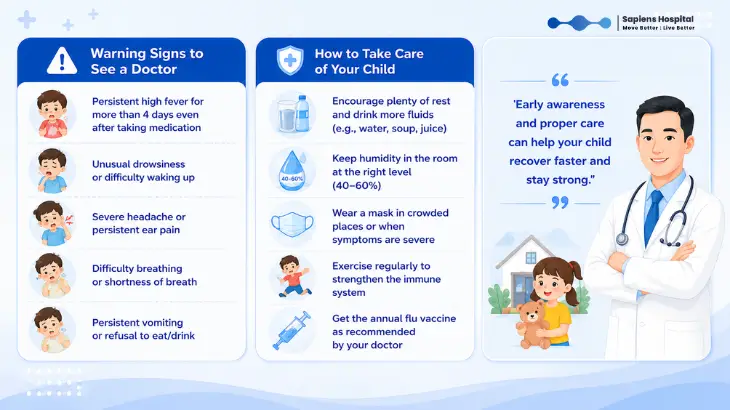
Red Flag Signs (Seek immediate medical attention if the cough is accompanied by):
- Prolonged fever or unexplained weight loss
- Night sweats or coughing up blood
- Rapid breathing or unusual shortness of breath
- Chest pain
- A clear history of choking before the cough started
- Chronic, excessive productive cough
- Recurrent pneumonia or failure to thrive (poor growth)
Diagnostic Tests for a Chronic Cough
A proper evaluation begins with a detailed medical history that goes far beyond asking "how many days has the child been coughing?"
A pediatrician will investigate:
- Is the cough dry or productive? Does it happen at night or during the day?
- Does it occur after running? Is there any wheezing?
- Are there nasal symptoms (congestion, runny nose, sneezing, itchy eyes)?
- Is there a history of fever, weight loss, or choking?
- Are there environmental triggers at home or school (secondhand smoke, pets, carpets, stuffed toys, dust, mold)?
Treatment for Allergy-Induced Chronic Cough
If the cough is linked to allergic rhinitis, treatment focuses on reducing nasal mucosal inflammation and postnasal drip. This may include:
- Proper nasal saline irrigation (saline washes)
- Specific antihistamines
- Intranasal corticosteroid sprays
- Strict avoidance of known allergens
⚠️ Key Takeaway: Allergy treatment requires time and consistency. Parents should not abruptly stop medications just because symptoms improve after a few days if the doctor has prescribed a continuous course, as controlling nasal inflammation effectively reduces the cough reflex and restores quality sleep.
Treatment for Pediatric Asthma
If the symptoms point to asthma, the physician will assess severity, symptom frequency, nighttime awakenings, rescue inhaler usage, activity limitations, and exacerbation history. Modern asthma management does not rely solely on rescue bronchodilators during an attack; instead, it prioritizes long-term controller medications to suppress airway inflammation, thereby preventing flare-ups and reducing long-term risks.
GINA emphasizes that comprehensive asthma care must include:
- Diagnostic confirmation
- Risk assessment
- Appropriate controller medications
- Patient/parent education on correct inhaler techniques
- Symptom monitoring and a personalized Asthma Action Plan
Household Triggers Parents Often Overlook
Children with allergy- or asthma-induced chronic coughs are far more sensitive to their environment than we realize. Common household triggers include:
- Dust and dust mites in mattresses, pillows, blankets, and plush toys
- Mold in damp bathrooms or unventilated walls
- Cigarette smoke (extremely hazardous) and incense smoke
- Perfume sprays and harsh chemical cleaning products with strong odors
- Pet dander and fur
- PM2.5 dust particles
Do Cough Medicines Help?
Cough syrups might make parents feel like they are actively treating the illness, but in cases of chronic cough, they do not address the root cause. If the cough stems from allergic rhinitis, the nose needs treatment. If it stems from asthma, the airways need control. If it is caused by chronic bronchitis, infection, or specific lung diseases, treatment must target those conditions.
Using multiple cough medicines consecutively without a diagnosis simply delays proper care. International guidelines firmly advocate for accurate diagnosis prior to therapy rather than relying on cough suppressants as a blanket solution.
Frequently Asked Questions (FAQs)
Q: Does a night cough always mean my child has asthma?
A: Not necessarily. Night coughing can be caused by allergic rhinitis, postnasal drip, asthma, GERD, or post-infectious bronchial hyperresponsiveness. However, if the night cough co-occurs with coughing after running, wheezing, chest tightness, or a family history of allergies, an asthma evaluation is highly recommended.
Q: Will a child with allergic rhinitis eventually develop asthma?
A: Not every child will, but nasal allergies and asthma are deeply connected. A child with allergic rhinitis—especially one who coughs after physical exertion, coughs at night, or experiences wheezing—should be evaluated for both conditions. It should not be dismissed as "just a simple nasal allergy."
Q: Does every child with a chronic cough need a chest X-ray?
A: Not always. For a cough lasting over 4 weeks, a pediatrician will decide based on history and physical findings. If red flag signs are present—such as chronic productive cough, prolonged fever, weight loss, shortness of breath, or abnormal lung sounds—a chest X-ray plays a vital role. Chronic cough guidelines advise targeted diagnostic testing rather than ordering tests indiscriminately.
Q: My child coughs every time they run. Should they stop exercising?
A: Absolutely not. Coughing after running can be a sign of exercise-induced bronchoconstriction or poorly controlled asthma. The child needs a proper medical evaluation and treatment. The ultimate goal of asthma care is to allow the child to exercise, play sports, and live a normal life—not to restrict their activities.
A chronic pediatric cough deserves careful attention, as it can range from poorly managed allergic rhinitis to asthma or other respiratory conditions. As a quick rule of thumb: if the cough is accompanied by nasal congestion, clear discharge, sneezing, itchy nose, and frequent throat-clearing, think allergic rhinitis. If it happens at night, after running, causes easy fatigue, chest tightness, or wheezing, think asthma. Keep in mind that a child can have both. Effective management does not mean "stopping the cough temporarily"—it means finding the root cause, controlling inflammation, eliminating triggers, mastering proper medication techniques, and ensuring continuous follow-up.
If your child has been coughing for more than 4 weeks, if the cough disrupts their sleep or exercise, or if it occurs alongside wheezing and other warning signs, please consult a pediatrician. Early, targeted care ensures your child sleeps better, plays harder, learns more effectively, and faces fewer flare-ups in the future.
⚠️ Emergency Warning: If your child exhibits severe breathing difficulties, blue-tinted lips (cyanosis), severe lethargy, blood in their cough, unexplained weight loss, chronic fever, or rapidly deteriorating symptoms, please go to the nearest emergency room immediately.
Sapiens Hospital
Move Better:Live Better
Tel. 02-111-3703
References
Chang AB, Oppenheimer JJ, Irwin RS, et al. Managing Chronic Cough as a Symptom in Children and Management Algorithms: CHEST Guideline and Expert Panel Report. CHEST. 2020.
Morice AH, Millqvist E, Bieksiene K, et al. ERS guidelines on the diagnosis and treatment of chronic cough in adults and children. European Respiratory Journal. 2020.
Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention, 2025 Update.
National Heart, Lung, and Blood Institute. 2020 Focused Updates to the Asthma Management Guidelines.
Bousquet J, et al. EAACI-endorsed ARIA 2024–2025 guidelines for allergic rhinitis.
Kanjanawasee D, et al. Chronic cough management: Practical guidelines and PICO-based evidence for treatment. 2024.
Related Content

When should a child with a high fever see a doctor? Learn the emergency red flags, dehydration signs, and febrile seizure care from SapienS Hospital.
10 Jul 2026

Is your child suffering from diarrhea and vomiting? Learn how to spot early signs of severe dehydration and manage fluid loss safely at home.
10 Jul 2026

If your child has a poor appetite, drops below weight and height standards, looks pale, gets sick frequently, or has chronic bowel issues—including difficulty swallowing, choking, vomiting, or persistent stomach pain—you should take them to see a doctor immediately.
10 Jul 2026