Hand, Foot, and Mouth Disease: Home Care Guide and Warning Signs
Last updated: 15 Jul 2026

Hand, Foot, and Mouth Disease: Home Care Guide and Warning Signs
Hand, Foot, and Mouth Disease (HFMD) is a common infectious disease that parents frequently hear about, especially during outbreaks in nurseries, kindergartens, or households with multiple young children. The typical progression often starts with a fever, sore mouth, decreased appetite, and drooling, followed by rashes or blisters on the palms, soles of the feet, around the mouth, or on the buttocks. Many families panic out of fear that the disease will become severe or lead to dangerous complications.
In reality, most cases of HFMD are mild and self-limiting, resolving on their own within 7–10 days, and the majority of children can be safely cared for at home. However, "mostly mild" does not mean "no need to be cautious." Some children—particularly very young infants, those who cannot drink water, or those infected with specific strains like Enterovirus 71 (EV-A71)—may have a higher risk of developing rare but severe complications affecting the nervous system, heart, or lungs. According to the CDC, HFMD is most common in children under 5 years old, highly contagious, and usually causes fever, mouth sores, and rashes on the hands and feet, with most patients improving on their own within 7–10 days.
What is Hand, Foot, and Mouth Disease?
Hand, Foot, and Mouth Disease (HFMD) is a viral infection caused by viruses in the Enterovirus genus, commonly affecting young children. The most frequent cause is Coxsackievirus A16. Another strain, Coxsackievirus A6, can cause more severe or widespread rashes. Enterovirus 71 (EV-A71) is a particularly significant strain in East and Southeast Asia because it is associated with more severe complications, such as encephalitis (brain inflammation), though these remain rare.
The name "Hand, Foot, and Mouth Disease" is sometimes confused with "Foot-and-Mouth Disease" (also called Hoof-and-Mouth Disease) found in livestock. However, these two diseases are completely unrelated. HFMD in children is caused by human-to-human viruses and is not transmitted by or to cattle, pigs, goats, or sheep, nor do common household pets spread this disease.
How Does It Spread?
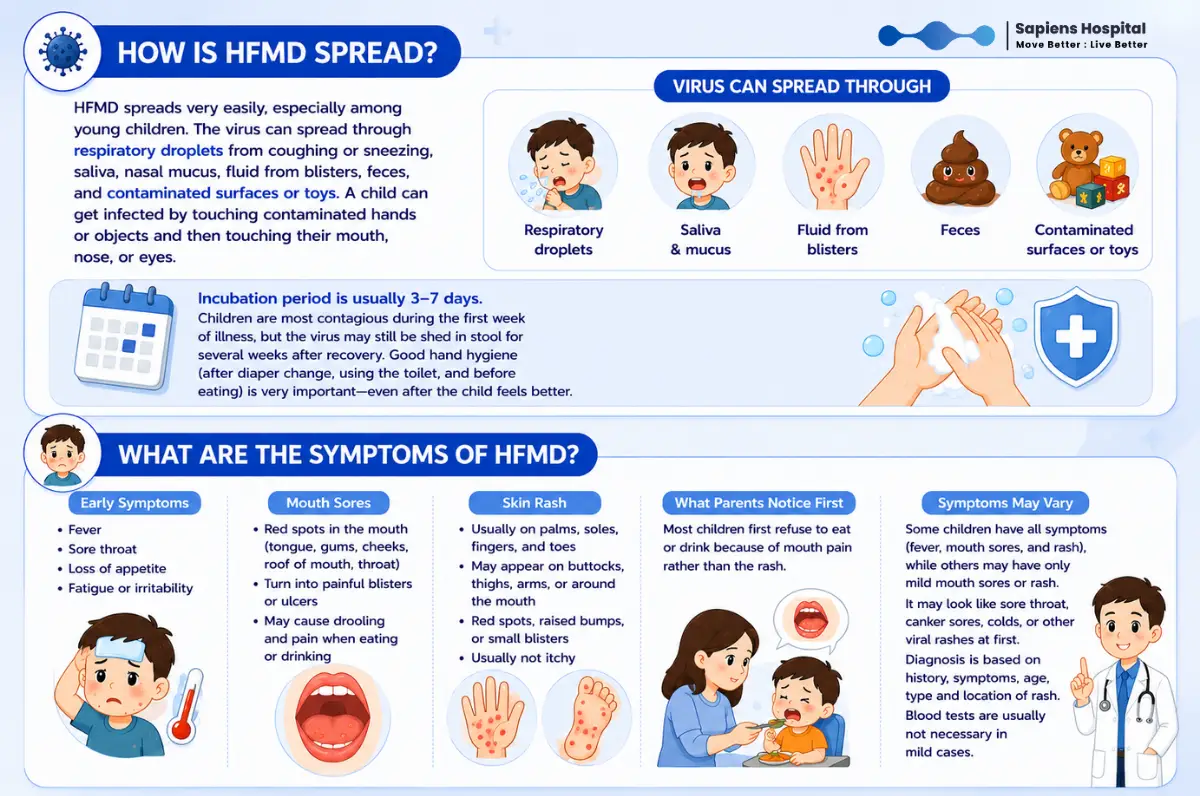
HFMD is highly contagious, especially among young children who share toys, frequently put their hands in their mouths, or have not yet developed proper hygiene habits. The virus spreads through:
The incubation period is typically 3–7 days. Infected children are most contagious during the first week of illness, but the virus can continue to shed in their stool for several weeks even after all symptoms have resolved. This is why thorough handwashing after changing diapers, using the restroom, and before eating is crucial, even if the child appears completely recovered.
What Are the Early Symptoms?
Children usually start with a fever, sore throat, loss of appetite, fatigue, or general irritability. Shortly after, mouth sores begin to appear. They often start as small red spots on the tongue, inner cheeks, roof of the mouth, or back of the throat, which then turn into painful blisters or ulcers. This pain causes children to refuse food or milk, drool excessively, or cry while swallowing.
Skin rashes typically appear on the palms, soles of the feet, fingers, and toes. Some children may also develop rashes on the buttocks, thighs, arms, or around the mouth. The rash may present as flat red spots, raised bumps, or small clear blisters. Generally, the skin rash is not very itchy or painful compared to the sores inside the mouth. The first thing parents usually notice is that "the child refuses to eat because of a sore mouth," rather than the rash on their hands and feet.
Some children present with the full triad of symptoms (fever, mouth sores, and rash), while others may only have mouth sores or a mild rash. In the early stages, it can easily be mistaken for pharyngitis, aphthous ulcers (canker sores), a common cold, or other viral rashes. Diagnosis is generally based on medical history, symptoms, the child's age, and the characteristic appearance and location of the rash and sores. In mild cases, blood tests or viral swabbing are rarely necessary.
Safe Home Care Guidelines
The cornerstone of HFMD home care is supportive treatment: managing symptoms, reducing fever, relieving pain, and preventing dehydration. There is no specific antiviral medication for general HFMD, and antibiotics are ineffective because the disease is viral, not bacterial. StatPearls notes that treatment for HFMD is primarily supportive, and currently, no antiviral drugs are approved specifically for treating this disease directly.
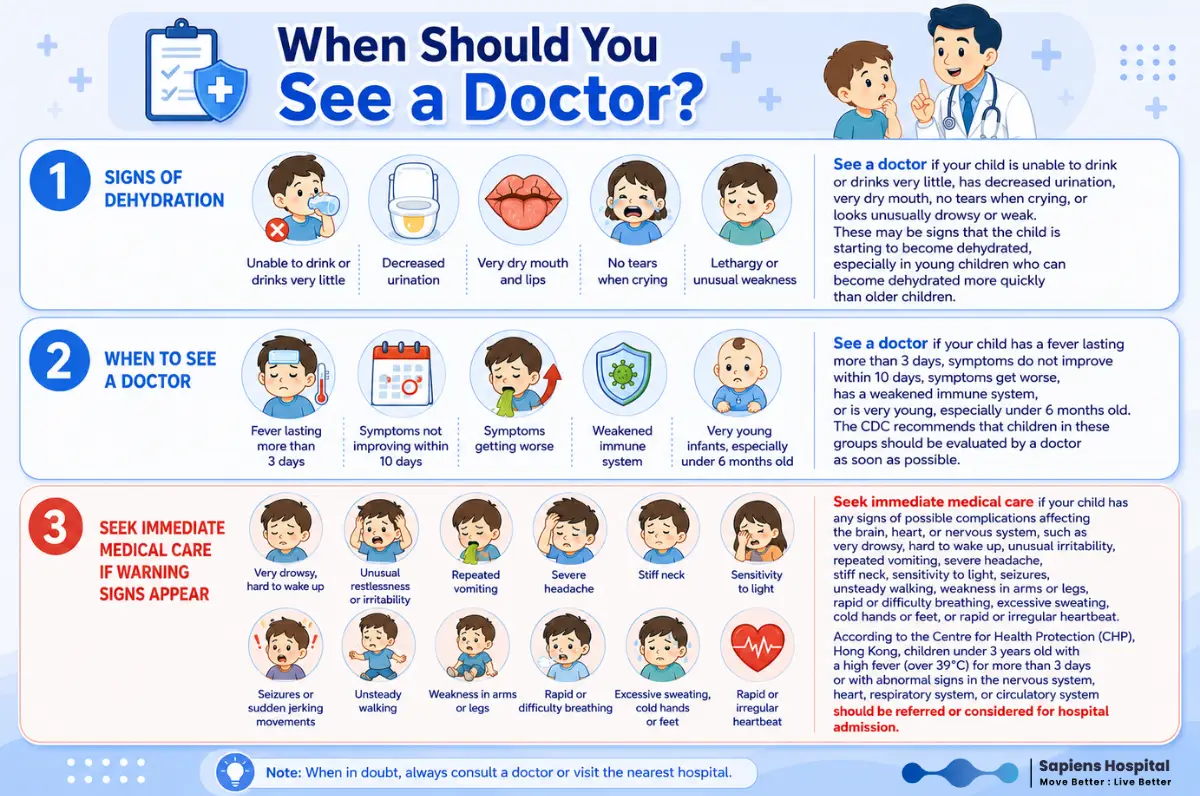
Children with painful mouth sores may completely refuse to drink fluids, even if they aren't vomiting or suffering from diarrhea. The CDC highlights dehydration as a common complication, especially in young children who find it difficult to swallow. Parents must closely monitor fluid intake and watch for signs of dehydration, such as decreased urination, a dry mouth, crying without tears, lethargy, or a significant drop in fluid consumption.
When to See a Doctor
Seek medical evaluation if your child:
Why Do Some Cases Become Severe?
While the vast majority of HFMD cases are mild, infections caused by certain strains—especially EV71—are associated with severe complications, including encephalitis, meningitis, myocarditis (heart muscle inflammation), acute flaccid paralysis, or neurogenic pulmonary edema (fluid in the lungs). Although these complications are rare, extra vigilance is required in East and Southeast Asia, where EV-A71 has historically caused severe outbreaks.
What makes severe cases dangerous is that they can start exactly like a typical, mild case of HFMD, but then deteriorate rapidly. Parents should not judge severity solely by the number of skin blisters, but rather by the child’s overall condition. Monitor whether the child is alert, able to drink fluids, breathing comfortably, interacting normally, and whether their symptoms are improving or worsening over time.
Frequently Asked Questions (FAQs)
Should I apply topical creams or pop the blisters?
No, you should never pop the blisters. The fluid inside contains live virus, and popping them increases the risk of spreading the infection to others or causing a secondary bacterial infection. Keep the skin clean and dry, and avoid scratching. If a blister pops naturally, wash it with clean water and mild soap, pat it dry, and monitor for signs of secondary infection, such as increased redness, warmth, swelling, pain, or pus.
If mouth sores are severe and the child cannot drink, a doctor may prescribe appropriate topical gels or oral pain relief based on the child's age. Avoid using over-the-counter numbing sprays (topical anesthetics) or herbal remedies without consulting a pediatrician, as they can cause swallowing difficulties, choking risks, or serious side effects in infants.
Is viral testing necessary?
For children with classic, mild symptoms, doctors usually diagnose HFMD based on a physical examination without requiring laboratory tests. However, if the child has severe symptoms, neurological or respiratory abnormalities, or if there is a suspected outbreak or a need to rule out other serious conditions, a doctor may collect throat swabs, stool samples, blister fluid, or cerebrospinal fluid for PCR testing. The CHP guidelines note that viral testing plays a vital role in cases with rapid deterioration, neurological complications, acute flaccid paralysis, or myocarditis.
How is HFMD different from chickenpox or allergic rashes?
HFMD typically presents with painful mouth ulcers paired with rashes on the palms and soles (and sometimes the buttocks). Chickenpox, on the other hand, presents with itchy, fluid-filled blisters at various stages of healing that spread across the torso, face, and scalp, and it rarely features the distinct, painful mouth ulcers seen in HFMD. Allergic rashes are usually very itchy and linked to specific foods, medications, or triggers, without the characteristic painful sore throat and pattern of blisters.
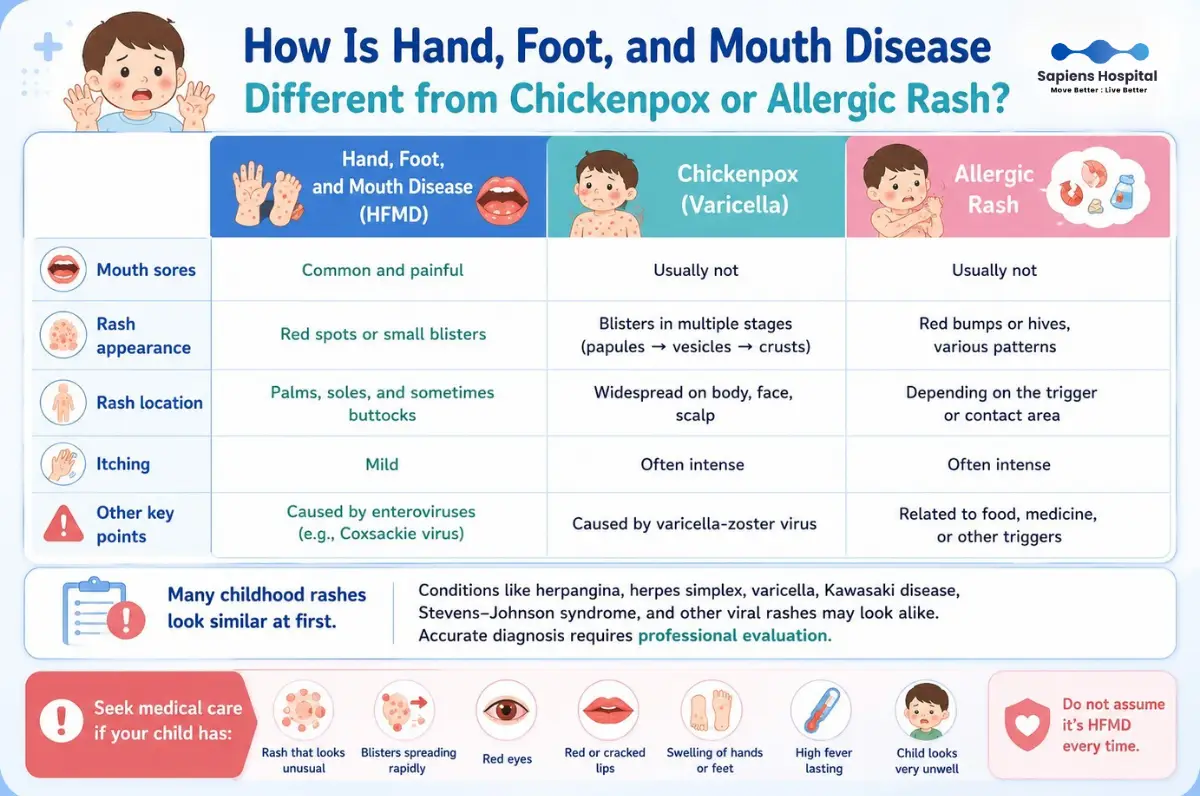
However, many childhood rashes look similar in their early stages (e.g., herpangina, herpes simplex, varicella, Kawasaki disease, Stevens-Johnson syndrome). According to StatPearls, differential diagnosis must account for various diseases presenting with oral ulcers and exanthems. If the rash looks unusual, spreads rapidly, or is accompanied by bloodshot eyes, bright red lips, swollen hands/feet, prolonged high fever, or severe illness, have a doctor examine the child immediately. Do not assume every rash is standard HFMD.
How many days should my child stay home from school?
Generally, children should stay home as long as they have a fever, severe mouth pain, uncontrollable drooling, weeping blisters, or still look visibly ill. This is the period when they are highly contagious and physically unready for activities. The CDC states that children may return to school or childcare once they are fever-free, feel well enough to participate in activities, and no longer have uncontrollable drooling. However, it is highly recommended to consult a healthcare provider or follow local school/community guidelines during an outbreak.
In an outbreak setting or in crowded daycare environments, policies may be stricter (e.g., requiring children to stay home until all blisters have completely dried up). The CHP recommends that symptomatic children avoid school and group activities, returning only after the fever has subsided and all blisters have crusted over, or in accordance with specific public health directives during an outbreak.
How can we prevent the virus from spreading at home and school?
The single most effective prevention method is frequent handwashing with soap and water, especially after changing diapers, using the toilet, blowing a child’s nose, wiping saliva, touching blister fluid, and before preparing or feeding meals.
Teach children proper handwashing habits and discourage them from putting their hands or toys in their mouths. Avoid sharing cups, utensils, towels, or personal items. The CDC recommends regular handwashing, cleaning and disinfecting frequently touched surfaces, and avoiding close contact (such as hugging, kissing, or sharing utensils) with infected individuals during their illness.
Toys, tables, chairs, doorknobs, bathrooms, and high-touch surfaces should be disinfected regularly, especially in homes with multiple children or immunocompromised individuals. The virus can survive on surfaces for some time, and since it sheds in stool for several weeks, strict hygiene must be maintained during diaper changes long after the fever is gone.
Can parents catch it? What precautions should adults take?
Yes, adults can contract HFMD. While many adults experience mild symptoms or no symptoms at all, they can still asymptomatically pass the virus to other children. Adult caregivers should practice strict hand hygiene, separate their personal items, avoid kissing the sick child, and regularly disinfect touched surfaces—especially if there are young infants, newborns, or immunocompromised individuals at home.
Pregnant women who come into contact with HFMD generally do not experience severe complications. However, they should contact their obstetrician if they develop symptoms or have concerns, as the situation depends on gestational age, baseline health, and the nature of the exposure. The CDC advises pregnant individuals to contact their healthcare provider if they think they may have been exposed to HFMD.
Quick Summary for Parents
Hand, Foot, and Mouth Disease (HFMD) is a common infectious disease that parents frequently hear about, especially during outbreaks in nurseries, kindergartens, or households with multiple young children. The typical progression often starts with a fever, sore mouth, decreased appetite, and drooling, followed by rashes or blisters on the palms, soles of the feet, around the mouth, or on the buttocks. Many families panic out of fear that the disease will become severe or lead to dangerous complications.
In reality, most cases of HFMD are mild and self-limiting, resolving on their own within 7–10 days, and the majority of children can be safely cared for at home. However, "mostly mild" does not mean "no need to be cautious." Some children—particularly very young infants, those who cannot drink water, or those infected with specific strains like Enterovirus 71 (EV-A71)—may have a higher risk of developing rare but severe complications affecting the nervous system, heart, or lungs. According to the CDC, HFMD is most common in children under 5 years old, highly contagious, and usually causes fever, mouth sores, and rashes on the hands and feet, with most patients improving on their own within 7–10 days.
What is Hand, Foot, and Mouth Disease?
Hand, Foot, and Mouth Disease (HFMD) is a viral infection caused by viruses in the Enterovirus genus, commonly affecting young children. The most frequent cause is Coxsackievirus A16. Another strain, Coxsackievirus A6, can cause more severe or widespread rashes. Enterovirus 71 (EV-A71) is a particularly significant strain in East and Southeast Asia because it is associated with more severe complications, such as encephalitis (brain inflammation), though these remain rare.
The name "Hand, Foot, and Mouth Disease" is sometimes confused with "Foot-and-Mouth Disease" (also called Hoof-and-Mouth Disease) found in livestock. However, these two diseases are completely unrelated. HFMD in children is caused by human-to-human viruses and is not transmitted by or to cattle, pigs, goats, or sheep, nor do common household pets spread this disease.
How Does It Spread?
HFMD is highly contagious, especially among young children who share toys, frequently put their hands in their mouths, or have not yet developed proper hygiene habits. The virus spreads through:
- Respiratory droplets from coughing or sneezing
- Saliva or nasal mucus
- Fluid from the blisters
- Feces
- Contaminated surfaces or toys
The incubation period is typically 3–7 days. Infected children are most contagious during the first week of illness, but the virus can continue to shed in their stool for several weeks even after all symptoms have resolved. This is why thorough handwashing after changing diapers, using the restroom, and before eating is crucial, even if the child appears completely recovered.
What Are the Early Symptoms?
Children usually start with a fever, sore throat, loss of appetite, fatigue, or general irritability. Shortly after, mouth sores begin to appear. They often start as small red spots on the tongue, inner cheeks, roof of the mouth, or back of the throat, which then turn into painful blisters or ulcers. This pain causes children to refuse food or milk, drool excessively, or cry while swallowing.
Skin rashes typically appear on the palms, soles of the feet, fingers, and toes. Some children may also develop rashes on the buttocks, thighs, arms, or around the mouth. The rash may present as flat red spots, raised bumps, or small clear blisters. Generally, the skin rash is not very itchy or painful compared to the sores inside the mouth. The first thing parents usually notice is that "the child refuses to eat because of a sore mouth," rather than the rash on their hands and feet.
Some children present with the full triad of symptoms (fever, mouth sores, and rash), while others may only have mouth sores or a mild rash. In the early stages, it can easily be mistaken for pharyngitis, aphthous ulcers (canker sores), a common cold, or other viral rashes. Diagnosis is generally based on medical history, symptoms, the child's age, and the characteristic appearance and location of the rash and sores. In mild cases, blood tests or viral swabbing are rarely necessary.
Safe Home Care Guidelines
The cornerstone of HFMD home care is supportive treatment: managing symptoms, reducing fever, relieving pain, and preventing dehydration. There is no specific antiviral medication for general HFMD, and antibiotics are ineffective because the disease is viral, not bacterial. StatPearls notes that treatment for HFMD is primarily supportive, and currently, no antiviral drugs are approved specifically for treating this disease directly.
- Fever and Pain Relief: You can use age- and weight-appropriate fever reducers/pain relievers, such as paracetamol or ibuprofen, following a doctor's advice or label instructions. Never give aspirin to children due to the risk of a rare but serious condition called Reye's syndrome. The CDC recommends over-the-counter medications to relieve fever and pain from mouth sores but explicitly warns against giving aspirin to children.
- Dietary Adjustments: Focus on "small amounts frequently" rather than forcing large meals. Children with mouth sores tolerate cold, soft, and non-irritating foods much better. Ideal options include cold milk, yogurt, cooled porridge, soft-boiled rice, soup, steamed egg, tofu, or soft, non-citrus fruits. Avoid hot, spicy, acidic foods, carbonated drinks, citrus juices, or crunchy/hard snacks, as these will sting the ulcers and make the child even more reluctant to drink fluids.
Children with painful mouth sores may completely refuse to drink fluids, even if they aren't vomiting or suffering from diarrhea. The CDC highlights dehydration as a common complication, especially in young children who find it difficult to swallow. Parents must closely monitor fluid intake and watch for signs of dehydration, such as decreased urination, a dry mouth, crying without tears, lethargy, or a significant drop in fluid consumption.
When to See a Doctor
Seek medical evaluation if your child:
- Cannot drink or drinks very little fluid.
- Urinates significantly less than usual, has a very dry mouth, or cries without tears.
- Becomes lethargic, unusually weak, or drowsy (signs of early dehydration, which develops faster in infants).
- Has a high fever lasting longer than 3 days.
- Does not improve within 10 days, or symptoms progressively worsen.
- Has an underlying immunodeficiency or is very young (especially under 6 months old, as the CDC recommends earlier medical assessment for this age group).
- Extreme lethargy, difficulty waking up, or unusual irritability.
- Persistent or projectile vomiting.
- Severe headache, stiff neck, or sensitivity to light (photophobia).
- Frequent myoclonic jerks (sudden body startles or twitches).
- Unsteady gait (ataxia) or sudden weakness in the arms or legs.
- Rapid breathing, shortness of breath, excessive sweating, cold hands/feet, or an abnormally fast heart rate.
Why Do Some Cases Become Severe?
While the vast majority of HFMD cases are mild, infections caused by certain strains—especially EV71—are associated with severe complications, including encephalitis, meningitis, myocarditis (heart muscle inflammation), acute flaccid paralysis, or neurogenic pulmonary edema (fluid in the lungs). Although these complications are rare, extra vigilance is required in East and Southeast Asia, where EV-A71 has historically caused severe outbreaks.
What makes severe cases dangerous is that they can start exactly like a typical, mild case of HFMD, but then deteriorate rapidly. Parents should not judge severity solely by the number of skin blisters, but rather by the child’s overall condition. Monitor whether the child is alert, able to drink fluids, breathing comfortably, interacting normally, and whether their symptoms are improving or worsening over time.
Frequently Asked Questions (FAQs)
Should I apply topical creams or pop the blisters?
No, you should never pop the blisters. The fluid inside contains live virus, and popping them increases the risk of spreading the infection to others or causing a secondary bacterial infection. Keep the skin clean and dry, and avoid scratching. If a blister pops naturally, wash it with clean water and mild soap, pat it dry, and monitor for signs of secondary infection, such as increased redness, warmth, swelling, pain, or pus.
If mouth sores are severe and the child cannot drink, a doctor may prescribe appropriate topical gels or oral pain relief based on the child's age. Avoid using over-the-counter numbing sprays (topical anesthetics) or herbal remedies without consulting a pediatrician, as they can cause swallowing difficulties, choking risks, or serious side effects in infants.
Is viral testing necessary?
For children with classic, mild symptoms, doctors usually diagnose HFMD based on a physical examination without requiring laboratory tests. However, if the child has severe symptoms, neurological or respiratory abnormalities, or if there is a suspected outbreak or a need to rule out other serious conditions, a doctor may collect throat swabs, stool samples, blister fluid, or cerebrospinal fluid for PCR testing. The CHP guidelines note that viral testing plays a vital role in cases with rapid deterioration, neurological complications, acute flaccid paralysis, or myocarditis.
How is HFMD different from chickenpox or allergic rashes?
HFMD typically presents with painful mouth ulcers paired with rashes on the palms and soles (and sometimes the buttocks). Chickenpox, on the other hand, presents with itchy, fluid-filled blisters at various stages of healing that spread across the torso, face, and scalp, and it rarely features the distinct, painful mouth ulcers seen in HFMD. Allergic rashes are usually very itchy and linked to specific foods, medications, or triggers, without the characteristic painful sore throat and pattern of blisters.
However, many childhood rashes look similar in their early stages (e.g., herpangina, herpes simplex, varicella, Kawasaki disease, Stevens-Johnson syndrome). According to StatPearls, differential diagnosis must account for various diseases presenting with oral ulcers and exanthems. If the rash looks unusual, spreads rapidly, or is accompanied by bloodshot eyes, bright red lips, swollen hands/feet, prolonged high fever, or severe illness, have a doctor examine the child immediately. Do not assume every rash is standard HFMD.
How many days should my child stay home from school?
Generally, children should stay home as long as they have a fever, severe mouth pain, uncontrollable drooling, weeping blisters, or still look visibly ill. This is the period when they are highly contagious and physically unready for activities. The CDC states that children may return to school or childcare once they are fever-free, feel well enough to participate in activities, and no longer have uncontrollable drooling. However, it is highly recommended to consult a healthcare provider or follow local school/community guidelines during an outbreak.
In an outbreak setting or in crowded daycare environments, policies may be stricter (e.g., requiring children to stay home until all blisters have completely dried up). The CHP recommends that symptomatic children avoid school and group activities, returning only after the fever has subsided and all blisters have crusted over, or in accordance with specific public health directives during an outbreak.
How can we prevent the virus from spreading at home and school?
The single most effective prevention method is frequent handwashing with soap and water, especially after changing diapers, using the toilet, blowing a child’s nose, wiping saliva, touching blister fluid, and before preparing or feeding meals.
Teach children proper handwashing habits and discourage them from putting their hands or toys in their mouths. Avoid sharing cups, utensils, towels, or personal items. The CDC recommends regular handwashing, cleaning and disinfecting frequently touched surfaces, and avoiding close contact (such as hugging, kissing, or sharing utensils) with infected individuals during their illness.
Toys, tables, chairs, doorknobs, bathrooms, and high-touch surfaces should be disinfected regularly, especially in homes with multiple children or immunocompromised individuals. The virus can survive on surfaces for some time, and since it sheds in stool for several weeks, strict hygiene must be maintained during diaper changes long after the fever is gone.
Can parents catch it? What precautions should adults take?
Yes, adults can contract HFMD. While many adults experience mild symptoms or no symptoms at all, they can still asymptomatically pass the virus to other children. Adult caregivers should practice strict hand hygiene, separate their personal items, avoid kissing the sick child, and regularly disinfect touched surfaces—especially if there are young infants, newborns, or immunocompromised individuals at home.
Pregnant women who come into contact with HFMD generally do not experience severe complications. However, they should contact their obstetrician if they develop symptoms or have concerns, as the situation depends on gestational age, baseline health, and the nature of the exposure. The CDC advises pregnant individuals to contact their healthcare provider if they think they may have been exposed to HFMD.
Quick Summary for Parents
| Can be managed at home if: | Go to the hospital IMMEDIATELY if: |
| * Child has a fever, mouth sores, and rash but can drink fluids well. | * Child cannot drink fluids, shows signs of dehydration, or passes very little urine. |
| * Child passes urine normally. | * Fever lasts more than 3 days. |
| * Child is alert, playful, and not lethargic. | * Child is lethargic, unusually drowsy, or difficult to wake. |
| * Symptoms are gradually improving day by day. | * Child experiences persistent vomiting, body jerks/twitches, unsteady walking, or limb weakness. |
| * Child has rapid breathing, cold hands/feet, or is under 6 months old. |
Sapiens Hospital
Move Better: Live Better
Tel. 02-111-3703
References:
Centers for Disease Control and Prevention. About Hand, Foot, and Mouth Disease.
Centers for Disease Control and Prevention. HFMD Symptoms and Complications.
Centers for Disease Control and Prevention. HFMD: Causes and How It Spreads.
Guerra AM, Orille E, Waseem M. Hand, Foot, and Mouth Disease. StatPearls. NCBI Bookshelf.
Centre for Health Protection, Department of Health, Hong Kong SAR. Management of Hand Foot Mouth Disease (HFMD) in Health Care Settings.
Related Content

Is your child suffering from diarrhea and vomiting? Learn how to spot early signs of severe dehydration and manage fluid loss safely at home.
10 Jul 2026

Youth sports injuries aren't limited to the limbs. Head impacts in football, basketball, rugby, cycling, skateboarding, gymnastics, or martial arts can cause a concussion.
10 Jul 2026

Is your child's leg or knee pain just a normal part of growing up, or is it a hidden sports injury?
Learn how to spot the crucial differences, identify medical red flags, and know exactly when to consult a doctor.
10 Jul 2026