Chronic Abdominal Pain: When Normal Test Results Do Not Mean "Nothing Is Wrong"

Chronic Abdominal Pain: When Normal Tests Do Not Mean "Nothing Is Wrong"
Chronic abdominal pain is a common problem that significantly impacts quality of life. Many patients suffer from symptoms for months or years, undergoing numerous tests—including blood work, ultrasounds, CT scans, MRIs, and gastrointestinal endoscopies—only to find no abnormalities to explain their condition.
In the past, we typically attributed pain to direct inflammation, infection, or organic dysfunction. Today, however, our understanding of chronic abdominal pain has changed significantly. Researchers have discovered that pain does not depend solely on an organ itself but also involves the complex interaction between the gut, the brain, the nervous system, and the immune system.
Not All Abdominal Pain Originates from the Stomach or Intestines
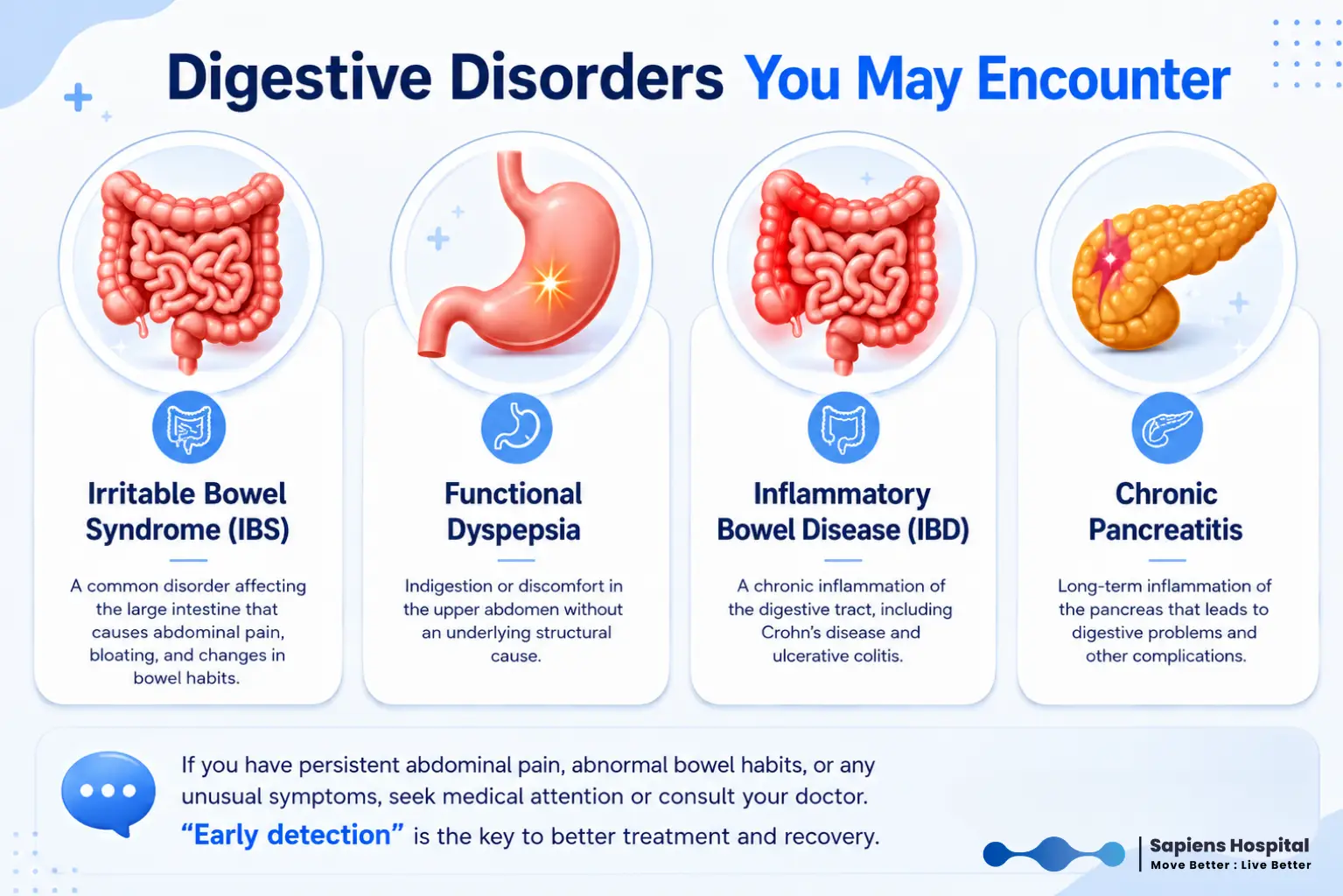
While gastrointestinal diseases remain major causes of chronic abdominal pain—such as Irritable Bowel Syndrome (IBS), Functional Dyspepsia, Inflammatory Bowel Disease (IBD), and Chronic Pancreatitis—many patients continue to experience pain even after the underlying disease has been treated or when tests show no clear abnormalities. Consequently, there is now a greater focus on the mechanisms of chronic pain, particularly the communication between the gut and brain, as well as changes in the nervous system related to pain perception.
Q&A: Why do I still have pain after all the tests?
One key concept gaining wider acceptance is the Gut-Brain Axis. The gut and brain are in constant communication. Stress, sleep deprivation, anxiety, or emotional states can affect gut function and pain perception. Conversely, gut dysfunction can affect a patient’s mood, sleep quality, and overall quality of life. This concept explains why some patients experience worsening symptoms during stressful periods or improvement when their overall health and sleep quality improve.
Q&A: Why does it hurt so much if test results are normal?
In recent years, there has been increasing evidence supporting Visceral Hypersensitivity. Patients in this group may have normal organ function but perceive stimuli as significantly more painful than the average person. This condition is common in patients with IBS and certain types of chronic abdominal pain syndromes, explaining why the severity of pain does not always correlate with test results.
When the Nervous System Becomes Hypersensitive
If pain persists for a long time, the nervous system responsible for processing pain can change. This condition is known as Central Sensitization. Once established, the intensity of the pain may no longer correlate with the severity of the original disease. Some patients continue to feel pain even after the underlying cause has resolved or test results have improved.
This condition also explains why some patients suffer from multiple types of pain simultaneously, such as:
- Chronic pelvic pain
- Chronic headaches
- Generalized musculoskeletal pain
While most people think of the stomach or intestines when they have abdominal pain, the source can sometimes be the abdominal wall or the nerves within the abdominal wall. Patients often describe the pain as burning, sharp, electric shock-like, or accompanied by numbness, and they can usually point to a specific, localized area. Examples include:
- Anterior Cutaneous Nerve Entrapment Syndrome (ACNES)
- Ilioinguinal/Iliohypogastric Neuralgia
For patients who can identify a clear, small point of tenderness on the abdominal wall, the possibility of abdominal wall pain should always be considered, as it is often misdiagnosed as an internal organ disorder.
Q&A: Are abdominal adhesions always the cause of pain?
Adhesions can occur after surgery or internal inflammation and are a significant cause of long-term bowel obstruction. However, the presence of adhesions does not always mean they are the cause of pain. In fact, many people have adhesions without symptoms, while others have severe pain that cannot be definitively linked to them. Additionally, surgical lysis of adhesions does not relieve pain in all patients and may lead to new adhesions.
Other Often-Overlooked Causes
- Thoracic Radiculopathy: Caused by irritation of the spinal nerve roots in the thoracic region, particularly T6-T12, which can cause pain in the rib cage or abdomen.
- Slipping Rib Syndrome: Caused by dysfunction of the cartilage of the lower ribs, leading to rib cage or under-rib pain, often mistaken for liver, gallbladder, or stomach disease.
The goal of diagnosis is not just to find a disease, but to understand the mechanism behind the pain. Some patients have direct organ issues, some have nerve or abdominal wall involvement, some have visceral hypersensitivity or central sensitization, and many have a combination of factors.
A thorough medical history, physical examination, and review of past tests remain the pillars of diagnosis. For patients suspected of having abdominal wall pain, doctors may use the Carnett’s Sign test to help differentiate abdominal wall pain from internal organ pain.
Treatment of Chronic Abdominal Pain
Modern treatment focuses not only on the underlying organ but also on the pain mechanisms behind it:
- Medications: Commonly used drugs include Amitriptyline, Duloxetine, Gabapentin, Pregabalin, and Mirogabalin. These help regulate nervous system function and reduce pain sensitivity.
- Nerve Blocks and Targeted Treatments: For nerve or abdominal wall pain, nerve blocks can assist in both diagnosis and treatment. In some cases, techniques like hydrodissection (guided by ultrasound) are used to release nerve compression.
- Internal Organ Pain Treatment: Specialized procedures, such as Celiac Plexus Blocks or Splanchnic Nerve Blocks, may be considered, particularly for patients with pancreatic cancer, chronic pancreatitis, or upper abdominal visceral pain.
We now know that the immune and nervous systems are closely linked through Neuroimmune Interaction. Immune cells can stimulate nerves to become hypersensitive, while nerves can influence inflammatory processes. This explains why patients still feel pain even after the disease is inactive—such as in patients with quiescent IBD or chronic pancreatitis.
The Future of Chronic Abdominal Pain Treatment
The focus is shifting from treating the organ alone to understanding the nervous system, leading to new technologies like Neuromodulation:
- Spinal Cord Stimulation: Traditionally used for other chronic pain, studies are increasingly looking at its use for chronic visceral pain.
- Vagus Nerve Stimulation: This nerve connects the brain to internal organs, including the digestive tract. It plays a role in controlling inflammation and autonomic nervous system function, making it a promising avenue for future research.
- Personalized Medicine: Since patients with similar symptoms may have vastly different causes—ranging from nerve issues to central sensitization—the future of treatment is moving toward a personalized approach rather than a "one-size-fits-all" method.


