Picky Eater, Slow Growth, and Not Gaining Weight: What Tests Are Needed?
Last updated: 13 Jul 2026

Picky Eater, Slow Growth, and Not Gaining Weight: What Tests Are Needed?
When parents feel that their child eats less than other children, isn't gaining weight, can wear the same clothing size for months, or when relatives comment on how small the child is, a wave of anxiety often follows. Questions quickly arise: “Is my child malnourished?” “Do they need a blood test?” “Is there a hidden disease?” or “Are they just a picky eater who will outgrow it?”
This cannot be answered with a one-size-fits-all approach. Some children eat very little but still grow consistently along their normal percentile curve, remain highly active, and have no underlying conditions. Conversely, some picky eaters drop off their growth curve, grow slowly, look pale, fatigue easily, suffer from chronic diarrhea, or fall ill frequently. The latter group requires a serious medical evaluation.
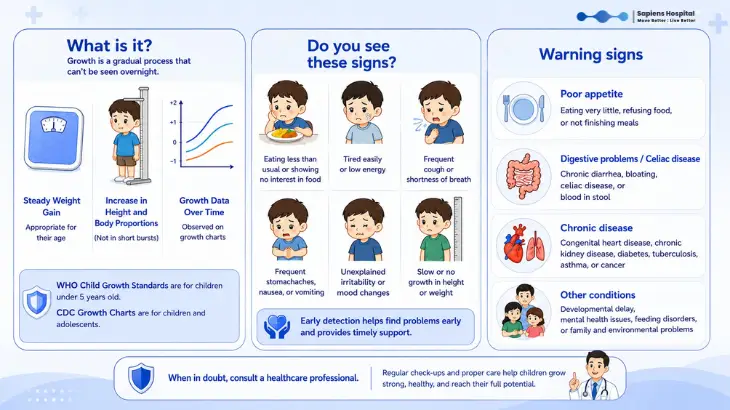
The most important takeaway is this: Do not rely on a single weight measurement or compare your child to others. Instead, look at the continuous "growth trend" of your own child on a standard growth chart.
The NICE guidelines use the term "Faltering Growth" to describe a downward trend in a child's growth. This is assessed by observing a drop in weight centiles combined with age, birth weight, height, BMI, and the overall clinical picture of the child. Similarly, the MSD Manual states that evaluating a child with slow weight gain should involve tracking weight, height (or length), and head circumference over time using standard growth charts (like WHO or CDC), alongside a detailed dietary history, family history, and a thorough physical examination.
Start with Growth Charts, Not Blood Tests
Not all small children have an underlying medical issue. Some are simply born small, have petite parents, and consistently follow their own growth curve. This is likely familial (genetic) short stature rather than malnutrition. However, if a child's weight was previously tracking on one curve and progressively drops across multiple centiles, or if their height growth begins to stall, doctors will prioritize this. Weight is usually the first indicator to change when a child receives insufficient calories, while a slowdown in height often reflects a more severe or prolonged issue.
For young children (under 5 years), the WHO Child Growth Standards—developed from data on 8,440 healthy children globally—serve as the primary benchmark. For older children, charts tracking age, gender, height, weight, and BMI are used to observe trends rather than isolated numbers.
Therefore, the very first step is to weigh the child, measure their height, measure head circumference (for infants), and accurately plot this data. Always bring your child’s vaccine book, health record, or previous weight logs to your appointment. Historical growth charts often provide more answers than an extensive panel of blood tests on day one.
Which Type of "Picky Eating" is Manageable, and When Should You See a Doctor?
Many toddlers and preschoolers go through a phase of picky eating, eating slowly, getting easily bored, or preferring play over food. If the child remains energetic, sleeps well, is not pale, has no diarrhea or vomiting, and their weight and height still follow their original curve, it might just be age-appropriate picky eating or a family feeding dynamic that needs behavioral adjustment rather than a sign of a serious illness.
However, you should seek a systematic medical evaluation if your child:
Main Causes of Poor Weight Gain
What Tests Should Be Done?
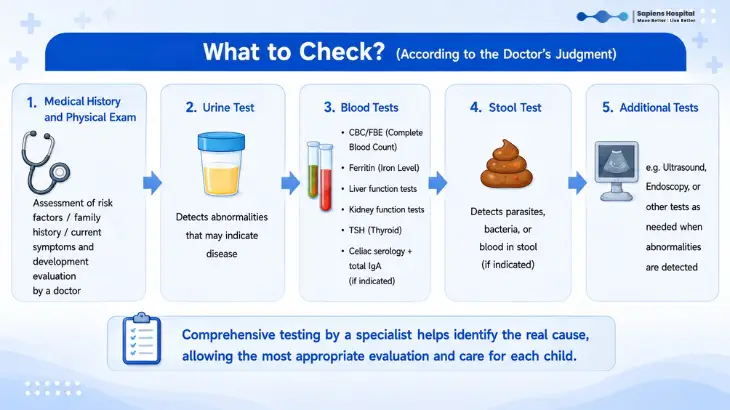
The most critical "test" on the first visit is a comprehensive history taking and physical examination. The doctor will ask about everything: pregnancy, birth weight, delivery, breastfeeding vs. formula, formula preparation, actual daily food intake, accepted textures, mealtime routines, who feeds the child, whether coercion or screens are used, vomiting, diarrhea, fevers, sleep, development, medications, underlying conditions, and the parents' physique.
The NICE guidelines recommend parents keep a food and behavior diary to give the doctor a realistic picture, rather than just stating the child "eats very little."
A physical examination goes beyond weight.
The doctor will assess height, body proportions, head circumference, signs of malnutrition, pallor, skin, hair, nails, oral cavity, teeth, abdomen, liver/spleen, heart, lungs, muscles, development, and signs of chronic diseases. A thorough exam dictates the direction of further testing, preventing aimless blanket testing.
Laboratory Tests:
In children with slow weight gain and specific clinical indications, doctors might consider a urine test and culture (especially in young children where a UTI might only present as slow weight gain). Basic blood panels might include a Complete Blood Count (CBC/FBE) and ferritin (for anemia/iron deficiency); electrolytes and kidney function; glucose; liver function; thyroid function (TSH); and celiac serology with total IgA if appropriate.
However, blood tests are not the first answer for every child. The AAP notes that lab tests or imaging should only be done if there are signs pointing to a specific problem, or if poor weight gain persists after appropriate interventions.
When to Check Stool or the Gastrointestinal Tract?
If a child isn't gaining weight and experiences chronic diarrhea, greasy/foul-smelling stools, severe bloating, chronic abdominal pain, frequent vomiting, blood/mucus in the stool, or eats a lot but doesn't grow, doctors will suspect malabsorption or intestinal inflammation. Stool tests can check for infections, parasites, or inflammatory markers. Endoscopies are generally reserved for severe cases or when weight continues to falter despite proper care.
When to Check Hormones or Height?
If the main issue is "poor weight gain" but height tracks normally, the focus is on caloric intake. But if height growth stalls, the child is unusually short for their age, bone age is delayed, puberty is late, or body proportions are abnormal, further evaluation of growth and hormones is needed.
Why Do Doctors Sometimes Avoid Extensive Blood Tests at First?
While comprehensive blood tests might bring peace of mind to parents, in children who are simply picky eaters and not gaining weight, excessive early testing often doesn't reveal the cause. If the history and physical exam don't point to a specific disease, asking the family to keep a 3-day food diary, observing mealtimes, adjusting caloric intake, and monitoring weight over an appropriate period often provides much better answers.
Initial Care Before and While Waiting to See a Doctor
If a child actually loses weight (not just fails to gain), seek medical attention sooner. Weight loss in children (past the newborn phase) is highly abnormal. See a doctor without waiting if your child is: Lethargic, weak, unable to eat, vomiting heavily, having chronic diarrhea, passing bloody stools, experiencing chronic fever, coughing chronically, having night sweats, breathing heavily, tiring easily, urinating abnormally, swollen (edema), extremely pale, falling sick recurrently, or showing developmental regression or clearly stalled height.
Frequently Asked Questions by Parents
Q: My child eats little but plays energetically. Do they need a blood test?
A: If weight and height follow their curve, development is normal, and there are no abnormal symptoms (diarrhea, fever, pallor), immediate blood tests may not be necessary. Doctors will start by reviewing growth charts and dietary habits.
Q: My child drinks a lot of milk but won't eat solid food.
What should I do?
A: Consult a doctor or pediatric dietitian to determine the appropriate amount of milk for their age. Excessive milk fills the child up, preventing them from feeling hungry for regular meals.
Q: If my child isn't gaining weight, should I give them dietary supplements?
A: Do not start oral nutritional supplements on your own without evaluating the cause. Some children just need caloric adjustments in regular food, some have underlying conditions to treat, and others need behavioral therapy. Supplements should be prescribed and monitored by a professional.
Q: Is my child small because the parents are small, or is it a disease?
A: Look at the growth trend and target height from the parents. A small child who grows consistently, is active, eats adequately, and has no other symptoms may just have a "familial small build." However, if they drop centiles or show symptoms like pallor or chronic diarrhea, further investigation is required.
Summary Do not judge your child's growth based solely on feelings or comparisons with other children. Start by accurately measuring weight, height, and head circumference, then plot them on a growth chart. Catching issues early helps differentiate between adjustable feeding behaviors and hidden diseases that need treatment. A child's growth isn't just a number on a scale; it's a vital sign of long-term health, energy, development, and quality of life.
Sapiens Hospital Move Better : Live Better Tel: 02-111-3703
References:
National Institute for Health and Care Excellence. Faltering growth: recognition and management of faltering growth in children. NICE Guideline NG75.
Royal Children’s Hospital Melbourne. Clinical Practice Guidelines: Slow weight gain.
World Health Organization. WHO Child Growth Standards: methods and development.
MSD Manual Professional Edition. Growth and Weight Faltering in Children.
American Academy of Pediatrics. Guidance on faltering weight in children.
When parents feel that their child eats less than other children, isn't gaining weight, can wear the same clothing size for months, or when relatives comment on how small the child is, a wave of anxiety often follows. Questions quickly arise: “Is my child malnourished?” “Do they need a blood test?” “Is there a hidden disease?” or “Are they just a picky eater who will outgrow it?”
This cannot be answered with a one-size-fits-all approach. Some children eat very little but still grow consistently along their normal percentile curve, remain highly active, and have no underlying conditions. Conversely, some picky eaters drop off their growth curve, grow slowly, look pale, fatigue easily, suffer from chronic diarrhea, or fall ill frequently. The latter group requires a serious medical evaluation.
The most important takeaway is this: Do not rely on a single weight measurement or compare your child to others. Instead, look at the continuous "growth trend" of your own child on a standard growth chart.
The NICE guidelines use the term "Faltering Growth" to describe a downward trend in a child's growth. This is assessed by observing a drop in weight centiles combined with age, birth weight, height, BMI, and the overall clinical picture of the child. Similarly, the MSD Manual states that evaluating a child with slow weight gain should involve tracking weight, height (or length), and head circumference over time using standard growth charts (like WHO or CDC), alongside a detailed dietary history, family history, and a thorough physical examination.
Start with Growth Charts, Not Blood Tests
Not all small children have an underlying medical issue. Some are simply born small, have petite parents, and consistently follow their own growth curve. This is likely familial (genetic) short stature rather than malnutrition. However, if a child's weight was previously tracking on one curve and progressively drops across multiple centiles, or if their height growth begins to stall, doctors will prioritize this. Weight is usually the first indicator to change when a child receives insufficient calories, while a slowdown in height often reflects a more severe or prolonged issue.
For young children (under 5 years), the WHO Child Growth Standards—developed from data on 8,440 healthy children globally—serve as the primary benchmark. For older children, charts tracking age, gender, height, weight, and BMI are used to observe trends rather than isolated numbers.
Therefore, the very first step is to weigh the child, measure their height, measure head circumference (for infants), and accurately plot this data. Always bring your child’s vaccine book, health record, or previous weight logs to your appointment. Historical growth charts often provide more answers than an extensive panel of blood tests on day one.
Which Type of "Picky Eating" is Manageable, and When Should You See a Doctor?
Many toddlers and preschoolers go through a phase of picky eating, eating slowly, getting easily bored, or preferring play over food. If the child remains energetic, sleeps well, is not pale, has no diarrhea or vomiting, and their weight and height still follow their original curve, it might just be age-appropriate picky eating or a family feeding dynamic that needs behavioral adjustment rather than a sign of a serious illness.
However, you should seek a systematic medical evaluation if your child:
- Persistently eats poorly and hasn't gained weight for months.
- Drops off their growth curve or shows stalled height.
- Looks pale, tires easily, or falls sick frequently.
- Has chronic diarrhea, vomiting, excessively greasy/foul-smelling stools, or blood in the stool.
- Suffers from chronic abdominal pain.
- Experiences difficulty swallowing, frequent choking, or coughing while being fed.
- Shows developmental delays.
- Displays severe feeding behavioral issues (e.g., extreme fear of certain textures, holding food in the mouth for a long time, or crying at every meal).
Main Causes of Poor Weight Gain
- Inadequate Caloric Intake (Most Common): The child might eat very small portions, lack a regular meal schedule, drink too much milk (and refuse solid food), or consume only sugary drinks and snacks. Sometimes, parents spoon-feed until the child fails to recognize hunger and fullness cues, or there are texture aversions (e.g., only accepting liquids, refusing to chew).
- Malabsorption or Nutrient Loss: The child eats enough, but the body cannot absorb the nutrients. Causes include chronic diarrhea, certain cow's milk protein allergies, celiac disease, inflammatory bowel disease, parasites, or specific pancreatic/gastrointestinal disorders. This group often presents with GI symptoms like frequent loose stools, abdominal pain, bloating, greasy/smelly stools, or blood in the stool.
- Increased Energy Expenditure: The body uses more energy than normal due to underlying conditions such as congenital heart disease, chronic lung disease, poorly controlled asthma, hyperthyroidism, chronic infections, kidney disease, liver disease, chronic inflammation, or (rarely) certain cancers.
What Tests Should Be Done?
The most critical "test" on the first visit is a comprehensive history taking and physical examination. The doctor will ask about everything: pregnancy, birth weight, delivery, breastfeeding vs. formula, formula preparation, actual daily food intake, accepted textures, mealtime routines, who feeds the child, whether coercion or screens are used, vomiting, diarrhea, fevers, sleep, development, medications, underlying conditions, and the parents' physique.
The NICE guidelines recommend parents keep a food and behavior diary to give the doctor a realistic picture, rather than just stating the child "eats very little."
A physical examination goes beyond weight.
The doctor will assess height, body proportions, head circumference, signs of malnutrition, pallor, skin, hair, nails, oral cavity, teeth, abdomen, liver/spleen, heart, lungs, muscles, development, and signs of chronic diseases. A thorough exam dictates the direction of further testing, preventing aimless blanket testing.
Laboratory Tests:
In children with slow weight gain and specific clinical indications, doctors might consider a urine test and culture (especially in young children where a UTI might only present as slow weight gain). Basic blood panels might include a Complete Blood Count (CBC/FBE) and ferritin (for anemia/iron deficiency); electrolytes and kidney function; glucose; liver function; thyroid function (TSH); and celiac serology with total IgA if appropriate.
However, blood tests are not the first answer for every child. The AAP notes that lab tests or imaging should only be done if there are signs pointing to a specific problem, or if poor weight gain persists after appropriate interventions.
When to Check Stool or the Gastrointestinal Tract?
If a child isn't gaining weight and experiences chronic diarrhea, greasy/foul-smelling stools, severe bloating, chronic abdominal pain, frequent vomiting, blood/mucus in the stool, or eats a lot but doesn't grow, doctors will suspect malabsorption or intestinal inflammation. Stool tests can check for infections, parasites, or inflammatory markers. Endoscopies are generally reserved for severe cases or when weight continues to falter despite proper care.
When to Check Hormones or Height?
If the main issue is "poor weight gain" but height tracks normally, the focus is on caloric intake. But if height growth stalls, the child is unusually short for their age, bone age is delayed, puberty is late, or body proportions are abnormal, further evaluation of growth and hormones is needed.
Why Do Doctors Sometimes Avoid Extensive Blood Tests at First?
While comprehensive blood tests might bring peace of mind to parents, in children who are simply picky eaters and not gaining weight, excessive early testing often doesn't reveal the cause. If the history and physical exam don't point to a specific disease, asking the family to keep a 3-day food diary, observing mealtimes, adjusting caloric intake, and monitoring weight over an appropriate period often provides much better answers.
Initial Care Before and While Waiting to See a Doctor
- Keep a 3-Day Food Diary: This is incredibly helpful for the doctor. Record it honestly (don't make it look better than reality). Note the time, food type, rough quantities, milk, water, sweet drinks, snacks, behaviors during meals, meal duration, and bowel movements/vomiting. This often reveals hidden issues, like grazing on snacks or lower total daily calories than assumed.
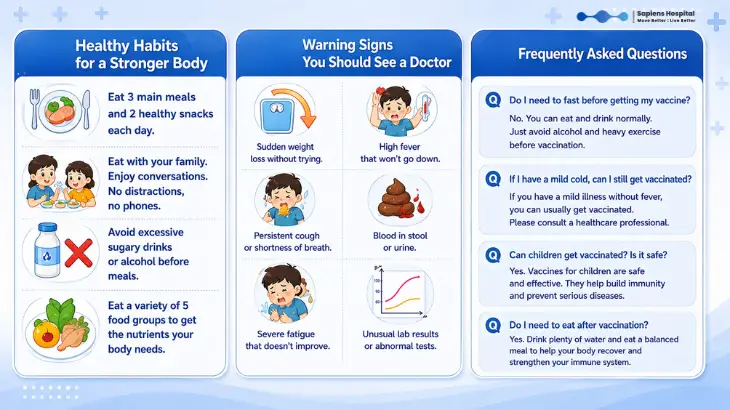
- Improve the Mealtime Environment: Create a relaxed atmosphere. Eat together as a family, maintain a consistent schedule (e.g., 3 main meals, 2 snacks), avoid forced feeding or punishment, and offer age-appropriate portions and textures.
- Watch the Milk Intake: A commonly overlooked issue is drinking too much milk. While nutritious, excessive milk (or high-energy drinks) can suppress the appetite for solid foods, a major contributor to faltering growth.
If a child actually loses weight (not just fails to gain), seek medical attention sooner. Weight loss in children (past the newborn phase) is highly abnormal. See a doctor without waiting if your child is: Lethargic, weak, unable to eat, vomiting heavily, having chronic diarrhea, passing bloody stools, experiencing chronic fever, coughing chronically, having night sweats, breathing heavily, tiring easily, urinating abnormally, swollen (edema), extremely pale, falling sick recurrently, or showing developmental regression or clearly stalled height.
Frequently Asked Questions by Parents
Q: My child eats little but plays energetically. Do they need a blood test?
A: If weight and height follow their curve, development is normal, and there are no abnormal symptoms (diarrhea, fever, pallor), immediate blood tests may not be necessary. Doctors will start by reviewing growth charts and dietary habits.
Q: My child drinks a lot of milk but won't eat solid food.
What should I do?
A: Consult a doctor or pediatric dietitian to determine the appropriate amount of milk for their age. Excessive milk fills the child up, preventing them from feeling hungry for regular meals.
Q: If my child isn't gaining weight, should I give them dietary supplements?
A: Do not start oral nutritional supplements on your own without evaluating the cause. Some children just need caloric adjustments in regular food, some have underlying conditions to treat, and others need behavioral therapy. Supplements should be prescribed and monitored by a professional.
Q: Is my child small because the parents are small, or is it a disease?
A: Look at the growth trend and target height from the parents. A small child who grows consistently, is active, eats adequately, and has no other symptoms may just have a "familial small build." However, if they drop centiles or show symptoms like pallor or chronic diarrhea, further investigation is required.
Summary Do not judge your child's growth based solely on feelings or comparisons with other children. Start by accurately measuring weight, height, and head circumference, then plot them on a growth chart. Catching issues early helps differentiate between adjustable feeding behaviors and hidden diseases that need treatment. A child's growth isn't just a number on a scale; it's a vital sign of long-term health, energy, development, and quality of life.
Sapiens Hospital Move Better : Live Better Tel: 02-111-3703
References:
National Institute for Health and Care Excellence. Faltering growth: recognition and management of faltering growth in children. NICE Guideline NG75.
Royal Children’s Hospital Melbourne. Clinical Practice Guidelines: Slow weight gain.
World Health Organization. WHO Child Growth Standards: methods and development.
MSD Manual Professional Edition. Growth and Weight Faltering in Children.
American Academy of Pediatrics. Guidance on faltering weight in children.
Related Content

Is your child's leg or knee pain just a normal part of growing up, or is it a hidden sports injury?
Learn how to spot the crucial differences, identify medical red flags, and know exactly when to consult a doctor.
10 Jul 2026

Youth sports injuries aren't limited to the limbs. Head impacts in football, basketball, rugby, cycling, skateboarding, gymnastics, or martial arts can cause a concussion.
10 Jul 2026

Childhood allergies can cause a chronic stuffy nose, runny nose, and snoring. Learn how to spot the symptoms, prevent sleep apnea, and treat your child.
10 Jul 2026